Respiratory
Respiratory
Here are the most common respiratory complaints you might encounter during your on call:
The most common ward call you’ll especially during the season, is to assess a patient with a chest infection such as acute bronchiolitis: Before assessing the patient, make sure you have gathered the relevant data about them including medications they’re on, when was the last dose, assess compliance and response to that medication, make sure you have seen their baseline examination and saturation and to compare it with their current presentation to assess whether the condition is stationary, improving or worsening.
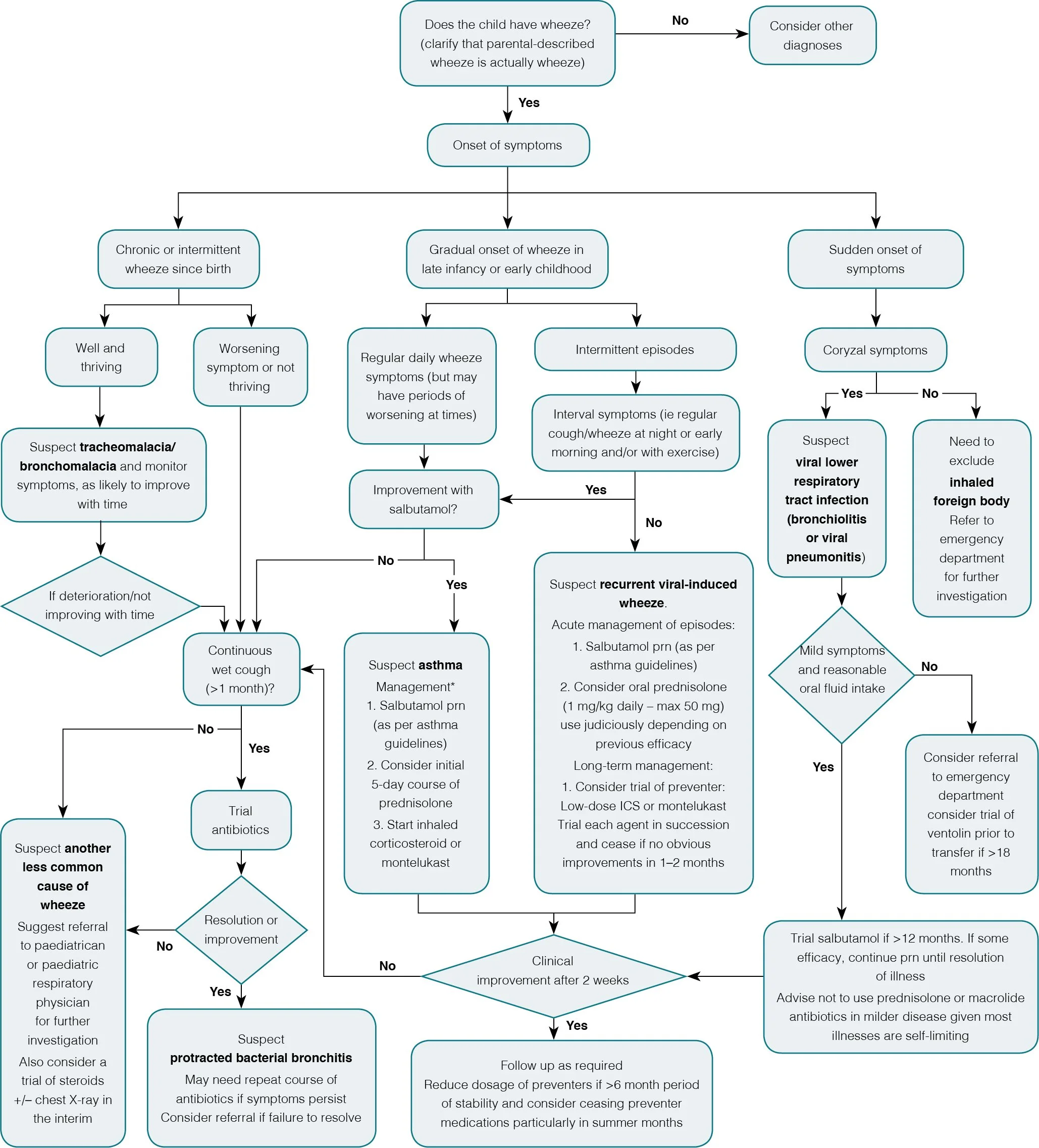
Follow the following steps to ensure a coherent approach to a wheezy or distressed child: If you are not sure, please always involve your senior.
1. Immediate Assessment and Stabilization
Assess ABCs:
Ensure airway is patent.
Check respiratory distress (retractions, nasal flaring, wheezing, SpO₂).
Assess circulation (heart rate, capillary refill).
Stabilize:
Administer oxygen to maintain SpO₂ > 92% - if not on oxygen already
Give inhaled salbutamol via spacer (2–4 puffs or nebulizer more commonly) every 20 minutes for up to 3 doses.
Add ipratropium bromide if moderate-to-severe wheeze.
Start oral prednisolone (1–2 mg/kg) or IV dexamethasone if severe.
2. Brief History and Examination
History:
Onset, triggers (infection, allergens), previous episodes, medications.
Examination:
Check for accessory muscle use, wheezing (expiratory or inspiratory), air entry, and associated symptoms (fever, cyanosis).
3. Investigations (if indicated)
Bedside:
Pulse oximetry, blood glucose.
Lab/Imaging:
Blood gas (if severe), CBC, CRP (if infection suspected), chest X-ray (if pneumonia or foreign body suspected). - these labs are mostly likely been done by the treating team earlier - make sure to see them to get a sense of the patients condition.
4. Management Based on Severity
Mild: Bronchodilators, oral steroids, and close monitoring.
Moderate-Severe:
Frequent nebulizers with bronchodilators and ipratropium.
IV magnesium sulfate if unresponsive.
Consider aminophylline or escalate to PICU for worsening condition.
5. Monitoring and Handover
Observe for clinical improvement (reduced respiratory distress, SpO₂ stabilization).
Communicate with the senior team and ensure a clear handover for ongoing care.